Body Care
Macular Degeneration
Jun
Macular degeneration sounds like something your laptop might do after too many software updates, but it is actually one of the most important eye health topics for adultsespecially after age 50. More formally called age-related macular degeneration, or AMD, this condition affects the macula, the small but mighty part of the retina responsible for sharp central vision. That is the vision you use to read a menu, recognize a friend’s face, thread a needle, drive safely, or spot the last slice of pie before someone else “accidentally” claims it.
The good news is that macular degeneration usually does not cause total blindness because side vision often remains. The less-good news is that central vision loss can seriously interfere with daily life. AMD can make straight lines look wavy, words look smudged, faces seem blurry, and low-light tasks feel like a poorly designed escape room. Understanding the symptoms, risk factors, diagnosis, treatment options, and day-to-day coping strategies can help protect vision and quality of life.
What Is Macular Degeneration?
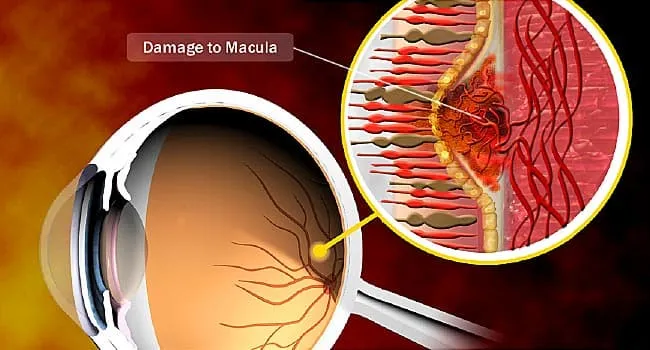
Macular degeneration is a progressive eye disease that damages the macula, which sits near the center of the retina at the back of the eye. The retina works like the camera sensor of the eye, collecting light and sending visual information to the brain. The macula handles fine detail and central focus. When it is damaged, the center of the visual field becomes blurry, distorted, dim, or missing.
People with macular degeneration may still notice movement and objects off to the side because peripheral vision is typically preserved. That means AMD rarely causes complete darkness. However, losing central vision can make everyday activities difficult, including reading, cooking, using a phone, watching television, shopping, managing medication labels, and recognizing facial expressions.
Dry vs. Wet Macular Degeneration
Macular degeneration is commonly divided into two major types: dry AMD and wet AMD. Both affect the macula, but they behave differently and require different management strategies.
Dry Macular Degeneration
Dry AMD is the more common form. It develops gradually as the macula thins with age and waste deposits called drusen collect under the retina. Many people with early dry AMD have no obvious symptoms at first. Over time, vision may become less sharp, colors may seem less vivid, and reading in dim light may become more difficult.
Dry AMD is often described in stages: early, intermediate, and late. In late dry AMD, some people develop geographic atrophy, an advanced form in which areas of retinal cells waste away. The name sounds like a map quiz nobody asked for, but it refers to patches of retinal damage that can expand and affect central vision.
Wet Macular Degeneration
Wet AMD is less common but usually more urgent. It happens when abnormal blood vessels grow under the retina and leak fluid or blood. This leakage can quickly damage the macula and cause sudden distortion or central vision loss. A person may notice that door frames, window blinds, or lines on a notebook look bent or wavy. Wet AMD is considered an advanced stage and should be evaluated promptly by an eye specialist.
Common Symptoms of Macular Degeneration
Early macular degeneration can be sneaky. It may sit quietly in the background while you blame blurry reading on bad lighting, tiredness, or the fact that restaurant menus are apparently printed for owls with magnifying glasses. As AMD progresses, symptoms become harder to ignore.
Common symptoms may include blurry or fuzzy central vision, straight lines appearing wavy, dark or empty spots in the center of vision, trouble recognizing faces, difficulty reading fine print, needing brighter light for close-up work, reduced color intensity, and slower adjustment when moving from bright light to dim rooms.
Any sudden change in vision deserves immediate medical attention. This is especially true if straight lines suddenly appear distorted, a new dark spot develops, or vision changes quickly in one eye. Wet AMD can progress rapidly, and earlier treatment may help preserve more vision.
Who Is Most at Risk?
Age is the biggest risk factor for macular degeneration. AMD is most common in adults over 50, and the risk rises with each decade. Still, age is not the only player in the game. Genetics, smoking, cardiovascular health, diet, and lifestyle can all influence risk.
Risk factors include being over age 50, having a family history of AMD, smoking or long-term exposure to tobacco smoke, high blood pressure, high cholesterol, obesity, cardiovascular disease, and a diet high in saturated fat. AMD is also reported more often in White adults, though people of all backgrounds can develop it.
Smoking deserves a special mention because it is one of the most important modifiable risk factors. In plain English: quitting smoking is one of the best gifts you can give your eyes. Your lungs will also send a thank-you card.
How Doctors Diagnose Macular Degeneration
A comprehensive dilated eye exam is the main way eye doctors detect macular degeneration. During the exam, drops widen the pupils so the doctor can see the retina and macula more clearly. The doctor may look for drusen, pigment changes, thinning tissue, fluid, bleeding, or other signs of retinal disease.
Several tests may be used. An Amsler grid can reveal distortion in central vision. Optical coherence tomography, often called OCT, creates detailed cross-sectional images of the retina and can show swelling, thinning, or fluid. In some cases, fluorescein angiography or OCT angiography may be used to evaluate blood flow and abnormal vessels.
Regular eye exams matter because AMD can begin before symptoms appear. Adults with risk factors, especially a family history of AMD, should ask an eye care professional how often they need retinal evaluation. Waiting until vision changes are obvious is a bit like waiting for smoke before checking whether the kitchen is on fire.
Treatment Options for Macular Degeneration
There is no universal cure for macular degeneration, but treatment and monitoring have improved dramatically. The best plan depends on the type and stage of AMD, the person’s overall health, and whether one or both eyes are affected.
AREDS2 Supplements for Intermediate AMD
For some people with intermediate dry AMD, eye doctors may recommend AREDS2 supplements. These supplements typically include vitamin C, vitamin E, zinc, copper, lutein, and zeaxanthin. They are not a magic shield, and they do not restore lost vision, but research has shown they can reduce the risk of progression to advanced AMD in certain patients.
People should not start high-dose eye vitamins without medical advice. Supplements can interact with health conditions, medications, and individual risk factors. For example, older formulas containing beta-carotene are generally avoided in current or former smokers because of lung cancer concerns. AREDS2 replaced beta-carotene with lutein and zeaxanthin.
Anti-VEGF Injections for Wet AMD
Wet AMD is commonly treated with anti-VEGF injections. VEGF stands for vascular endothelial growth factor, a protein that encourages abnormal blood vessels to grow and leak. Anti-VEGF medications help block that process. These medicines are injected into the eye after numbing drops are applied.
The idea of an eye injection makes many people want to sprint dramatically into the sunset. In practice, patients often report that the procedure is quicker and less uncomfortable than expected. Treatment may need to be repeated regularly, and the schedule varies depending on the medication and the eye’s response. The goal is to reduce leakage, stabilize vision, and sometimes improve vision.
Newer Treatments for Geographic Atrophy
For geographic atrophy, a late form of dry AMD, newer injectable treatments have been approved in recent years to slow the growth of retinal damage. These treatments target part of the immune system known as the complement pathway. They are not designed to bring back vision that has already been lost, but they may slow progression in appropriate patients.
Because these medicines require ongoing eye injections and carry potential risks, the decision to use them should be made with a retina specialist. The conversation usually includes expected benefits, treatment burden, safety considerations, and the patient’s personal goals.
Lifestyle Habits That May Help Protect Vision
Healthy habits cannot guarantee that macular degeneration will not develop or progress, but they can support eye health and overall health. The retina depends on good blood flow, oxygen, and nutrients, so the same habits that help the heart often help the eyes.
Helpful strategies include not smoking, eating a diet rich in leafy greens and colorful vegetables, choosing fish or other sources of omega-3 fatty acids when appropriate, managing blood pressure and cholesterol, exercising regularly, maintaining a healthy weight, wearing sunglasses that block UV light, and keeping scheduled eye exams.
Think of it as a retirement plan for your retinas. You may not see the payoff instantly, but future you may be very grateful.
Living With Macular Degeneration
Macular degeneration changes how people use their vision, but it does not have to erase independence. Low-vision rehabilitation can teach practical strategies for reading, cooking, using technology, navigating safely, and organizing the home. Magnifiers, high-contrast labels, large-print books, voice assistants, screen readers, brighter task lighting, and smartphone accessibility settings can make daily life easier.
Small changes often help. Put contrasting tape on stair edges. Use bold markers for labels. Choose clocks and phones with large numbers. Place frequently used items in consistent locations. Add lighting where tasks happen, not just where lamps look stylish. A beautiful lamp across the room is nice, but a bright task light next to the pill organizer is the real MVP.
Emotional support also matters. Vision changes can cause frustration, anxiety, grief, and isolation. Joining a support group, talking with a counselor, and involving family members can make adaptation less lonely. AMD is a medical condition, not a character flaw. Needing tools, help, or extra time is not “giving in”; it is smart problem-solving.
When to Call an Eye Doctor
Call an eye doctor promptly if you notice sudden blurring, new distortion, a dark spot in central vision, difficulty reading that appears suddenly, or a major change in one eye. If you already have AMD in one eye, report changes in the other eye right away. Wet AMD can move quickly, and time matters.
For ongoing monitoring, many doctors recommend using an Amsler grid at home. This simple grid can help reveal new distortion. Cover one eye at a time, look at the center dot, and notice whether lines look wavy, missing, or blurred. If the grid changes, contact your eye care team.
Practical Experiences Related to Macular Degeneration
Living with macular degeneration is not just a medical story; it is a kitchen-table, grocery-aisle, phone-screen, birthday-card story. Many people first notice AMD in small, ordinary moments. A grandmother may realize she can still see her grandchild running across the yard, but the child’s face looks blurry when standing directly in front of her. A retired teacher may notice that the center of a word disappears while reading, as though the page is playing hide-and-seek. A driver may see street signs less clearly and decide, wisely, to avoid night driving.
One common experience is the “lighting upgrade.” People with AMD often discover that what used to count as enough light no longer does the job. Reading a recipe may require a bright lamp placed directly over the counter. Restaurant menus may need a phone flashlight. Medication bottles may need large-print labels or a magnifying glass. This can feel annoying at first, but the right lighting setup can restore confidence quickly.
Another experience is learning to use peripheral vision more intentionally. Since AMD affects central vision, some people are taught eccentric viewing techniques, which involve looking slightly away from an object so a healthier part of the retina can help. It feels unnatural at firstlike trying to read a text message by politely ignoring itbut with practice, it can help with reading, recognizing shapes, and completing close-up tasks.
Technology can become a powerful ally. Smartphones can enlarge text, read messages aloud, identify objects, increase contrast, and turn speech into written notes. Tablets and e-readers allow large fonts and high-contrast backgrounds. Audiobooks can bring back the pleasure of reading when printed pages become tiring. Voice assistants can set reminders, read weather updates, and help with shopping lists. The best device is not always the fanciest one; it is the one the person actually uses without wanting to throw it into a drawer forever.
Family communication is another major part of the experience. Loved ones may not understand why someone with AMD can see a chair across the room but cannot read a label directly in front of them. Explaining central vision loss helps reduce confusion. A simple phrase can help: “I still have side vision, but the middle of what I look at is blurry.” That one sentence can prevent a surprising number of misunderstandings.
People receiving eye injections for wet AMD often describe their first appointment as the scariest. The word “injection” does not exactly bring confetti energy. But after numbing drops, careful cleaning, and a quick procedure, many patients say the anticipation was worse than the treatment. The bigger challenge is often keeping up with appointments, arranging transportation, and staying consistent even when vision feels stable.
Macular degeneration also teaches patience. Tasks may take longer. Reading may require breaks. Cooking may need better organization. But adaptation is not defeat. It is a new operating system for daily life. With medical care, low-vision tools, healthy habits, and support, many people continue to enjoy hobbies, relationships, travel, and independence. The goal is not to pretend nothing has changed. The goal is to build a life where vision changes do not get the final word.
Conclusion
Macular degeneration is a common eye disease that affects central vision, especially in adults over 50. It can make reading, driving, recognizing faces, and seeing fine details more difficult, but early detection and proper care can make a meaningful difference. Dry AMD often progresses slowly, while wet AMD can cause faster vision changes and usually needs prompt treatment. Regular eye exams, healthy lifestyle choices, AREDS2 supplements when recommended, anti-VEGF treatment for wet AMD, newer options for geographic atrophy, and low-vision support can all play a role in protecting independence and quality of life.
The most important takeaway is simple: do not ignore changes in central vision. If lines look wavy, words disappear, or a dark spot shows up in the middle of what you see, call an eye care professional. Your macula may be small, but it has a very big joband it deserves excellent care.
